Early detection of ectopic pregnancy via ultrasound can prevent complications. Learn the key signs, symptoms, and what to expect during an ultrasound scan.
By Shubhra Mishra — a mom of two who turned her own confusion during pregnancy into BumpBites, a global mission to make food choices clear, safe, and stress-free for every expecting mother. 💛
Check whether any food is safe during pregnancy with the BumpBites Food Safety Checker.
Download the Complete Pregnancy Food Guide (10,000 Foods) 📘
Instant PDF download • No spam • Trusted by thousands of moms
💡 Your email is 100% safe — no spam ever.
Quick take: An ectopic pregnancy can often be spotted on a transvaginal ultrasound by the presence of an empty uterus, an adnexal mass, or a gestational sac located outside the uterine cavity. The best chance of catching it early is to have the scan done as soon as you have a positive pregnancy test and any concerning symptoms, especially if your hCG levels are rising faster than expected. If the ultrasound looks normal but you still feel pain or notice bleeding, contact your provider right away.
It’s 3 a.m., you’ve just risen from a restless night, and a sharp lower‑abdominal ache makes you wonder if something’s wrong. You’ve taken a pregnancy test, it’s positive, and now the question that keeps looping in your mind is: “Is this pregnancy in the right place?” You’re not alone—many expecting parents face the same worry, and the answer often lies in an early ultrasound.
In this guide we’ll walk through what an ectopic pregnancy looks like on an ultrasound, when the scan should be done, how accurate it is, and what the findings mean for your care. We’ll also explain how hCG levels, risk factors, and the type of ultrasound machine influence what you and your provider see. By the end you’ll know the key signs to watch for, the limits of imaging, and the next steps if something looks off.
Whether you’re navigating a surprise positive test, coping with unexplained pain, or simply preparing for your first prenatal visit, the information below will help you feel more confident about the role of ultrasound in early ectopic pregnancy detection.
What are the early ultrasound signs of ectopic pregnancy?
Early ultrasound clues are subtle but distinct. The most common findings include an empty uterine cavity when a gestational sac should be visible, a tubal or adnexal mass that may appear as a “ring of fire” on Doppler, and the absence of a fetal pole where it belongs. The gestational sac, when present, is usually located outside the endometrial lining—often in the fallopian tube, but occasionally in the abdomen or ovary.
These signs are most reliable when the sonographer systematically sweeps both sides of the pelvis and correlates the images with the patient’s quantitative hCG level. Even a faint peripheral blood flow signal can tip the balance toward an urgent work‑up, highlighting why timely scanning is essential.
Adnexal mass or “ring of fire”
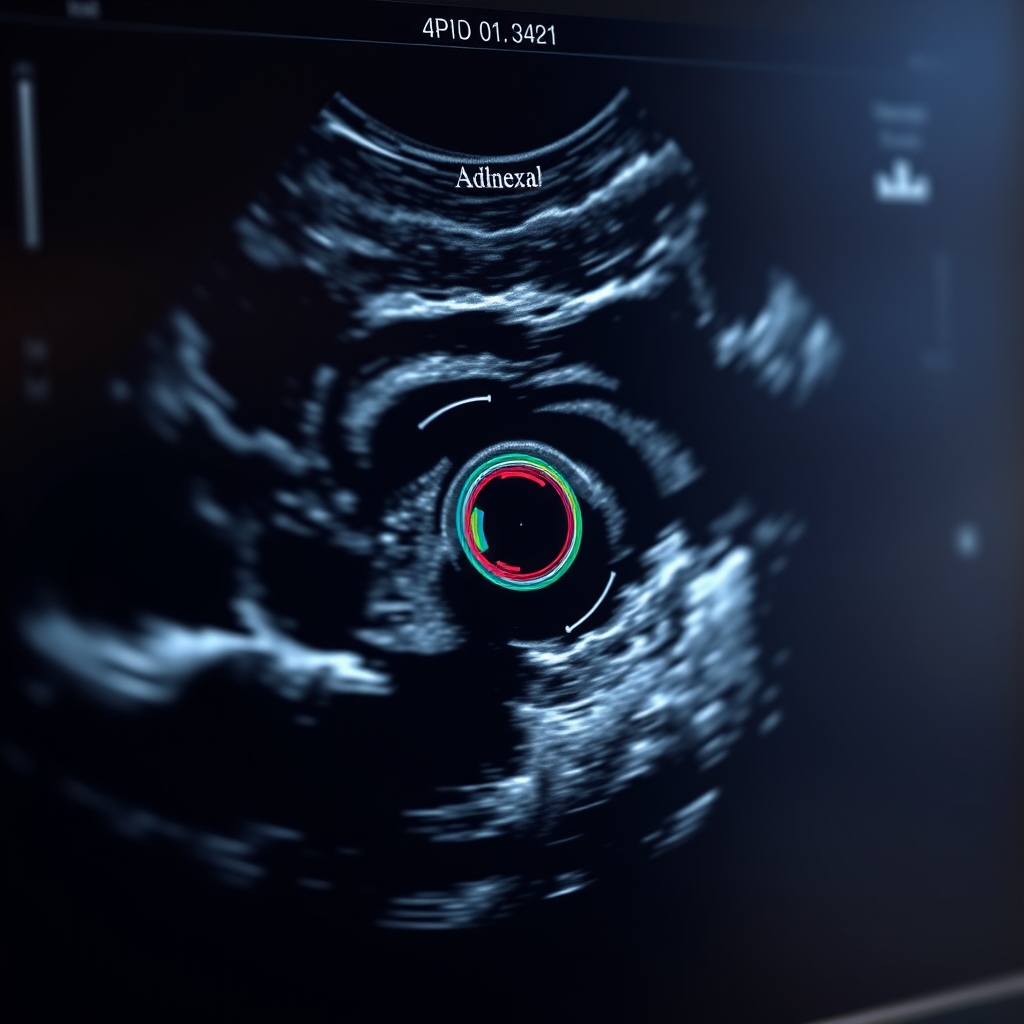
On a transvaginal scan, an ectopic pregnancy often shows a hypoechoic (dark) mass near the ovary with peripheral blood flow. Color Doppler highlights increased vascularity, giving the classic “ring of fire” appearance. This sign is sensitive but not exclusive—ovarian cysts can look similar, so the clinical picture matters.
Empty uterus
If the uterus looks completely empty despite a rising hCG level (usually >1500 mIU/mL), the suspicion for ectopic pregnancy rises sharply. A normal intrauterine pregnancy at that hCG level should already show a gestational sac with a yolk sac.
Abnormal gestational sac location
When a sac is visualized outside the uterine cavity, the diagnosis becomes clear. The sac may be seen within the ampullary portion of the tube (most common) or, less frequently, in the abdominal cavity. In abdominal ectopics the sac can be surrounded by free fluid and may be larger because it has more space to grow before rupture.
Absence of fetal pole
In a normal pregnancy, the fetal pole appears by about 5‑6 weeks gestation. Its absence when the hCG is high enough to expect a pole suggests an abnormal implantation.
These signs often appear alongside early symptoms such as unilateral pelvic pain, vaginal spotting, or shoulder pain from intra‑abdominal bleeding. Recognizing the ultrasound pattern together with the clinical picture speeds up diagnosis and treatment.
Because the early ectopic can be tiny, radiologists rely on a systematic sweep of the adnexa and a careful comparison with the patient’s hCG values. Even a subtle peripheral blood flow signal can tip the balance toward an urgent work‑up, highlighting why timely scanning is essential.
Typical “ring of fire” sign on a transvaginal scan.
How is ectopic pregnancy diagnosed with transvaginal ultrasound?
Transvaginal ultrasound (TVUS) is the gold‑standard imaging tool for early pregnancy assessment. By placing a high‑frequency probe just inside the vagina, clinicians obtain a close view of the uterus and adnexa, often detecting an ectopic pregnancy as early as 4–5 weeks gestation.
Accurate diagnosis also depends on the sonographer’s experience and on coordinating the scan with serial hCG measurements. When the imaging and lab data align, confidence in the diagnosis rises dramatically, allowing for timely, less invasive treatment.
Step‑by‑step diagnostic process
Confirm intrauterine gestational sac: The sonographer first looks for a sac inside the endometrial cavity. If none is seen, suspicion rises.
Assess adnexal region: The probe is angled to visualize the fallopian tubes and ovaries. A tubal mass, free fluid, or the “ring of fire” can be identified.
Measure hCG trends: The scan is paired with quantitative hCG testing. A level above 1500–2000 mIU/mL without an intrauterine sac is a red flag.
Apply discriminatory zone: ACR and ACOG define a “discriminatory zone” where a uterus should be visible; exceeding it without a sac suggests ectopic.
Document findings: Images and measurements are saved for review, and the team discusses management options.
Why transvaginal beats abdominal ultrasound early on
Abdominal (transabdominal) ultrasound uses a lower‑frequency probe placed on the abdomen. It provides a broader view but less detail, making it harder to spot a tiny tubal mass before 6 weeks. TVUS therefore detects ectopic pregnancies roughly a week earlier on average, which can be crucial for preventing rupture.
Best ultrasound machine for detecting ectopic pregnancy
High‑resolution machines with linear transducers (7–12 MHz) and advanced Doppler capabilities improve visualization of small masses and blood flow. Brands commonly used in obstetrics—GE Voluson, Philips EPIQ, and Siemens Acuson—meet the standards set by the American College of Radiology. While a top‑tier device isn’t required for a diagnosis, facilities with newer technology often report slightly higher detection rates.
Prompt referral to a center with experienced sonographers and up‑to‑date equipment can shave days off the diagnostic timeline, giving you more treatment options and a lower chance of emergency surgery.
Difference between tubal and abdominal ectopic pregnancy on ultrasound
Most ectopic pregnancies implant in the fallopian tube (≈95 %). Abdominal implantations are rare but carry a higher risk of massive hemorrhage because the surrounding tissue cannot contract to limit bleeding.
Feature
Tubal ectopic
Abdominal ectopic
Typical location
Fallopian tube, often ampullary
Peritoneal cavity, near bowel or omentum
Ultrasound appearance
Adnexal mass, “ring of fire,” possible free fluid
Irregular sac not attached to uterus, may be larger, variable vascularity
Gestational age at detection
4–6 weeks
6–8 weeks (often later due to space)
Risk of rupture
10–15 % before 7 weeks
Higher, often >20 %
Management
Medical (methotrexate) or surgical (laparoscopy)
Usually surgical (laparotomy) due to location
Both types can be identified on TVUS, but abdominal ectopics sometimes require additional imaging (e.g., MRI) if the sac is deep in the pelvis or obscured by bowel gas.
The clinical implications differ: tubal ectopics often respond to methotrexate if caught early, whereas abdominal ectopics usually need operative removal because the blood supply is less predictable. Knowing the exact location from the scan helps your care team choose the safest approach.
When should I get an ultrasound if I suspect ectopic pregnancy?
Timing is key. If you have a positive home pregnancy test and any of the following—sharp pelvic pain, vaginal spotting, or a sudden drop in hCG—you should schedule a TVUS promptly, ideally within 24–48 hours. Early detection (before 6 weeks) gives the widest range of treatment options, including medical management.
Waiting too long can narrow the window for methotrexate and increase the chance of rupture, which often requires emergency surgery. If you notice any new or worsening symptoms, call your clinic right away and ask for an urgent scan.
How early can an ectopic pregnancy be detected with ultrasound?
Transvaginal scans can reveal a tubal mass as early as 4 weeks gestation, especially when hCG levels are above the discriminatory zone (≈1500 mIU/mL). By 5–6 weeks, most ectopic pregnancies will show a clear adnexal mass or an empty uterus with rising hCG.
How long does it take for ectopic pregnancy to show on ultrasound?
In most cases the gestational sac becomes visible within a week after the hCG crosses the discriminatory threshold. However, if the pregnancy is very early or the patient has a high body mass index (BMI), the mass may not be seen for several days, necessitating repeat scanning.
What if the ultrasound is normal but symptoms persist?
A normal scan does not always rule out an ectopic pregnancy. Persistent pain, worsening spotting, or an hCG rise that outpaces the expected doubling can signal a false‑negative scan. In such situations, clinicians often repeat the TVUS in 48 hours or order a serial hCG test to track the trend.
Insurance plans in the U.S. and the NHS in the UK typically cover repeat scans when a provider documents ongoing concern, but it’s worth confirming coverage ahead of time so you aren’t surprised by a bill.
Can a normal ultrasound miss an ectopic pregnancy?
Yes. False‑negative results occur in up to 10 % of cases, according to ACOG guidelines. Reasons include very early gestational age, suboptimal probe placement, obesity, and atypical implantation sites (e.g., interstitial or cervical ectopics). A “normal” scan should be interpreted alongside clinical findings and hCG trends.
Because the early ectopic can be minute, a skilled sonographer will often repeat the exam if the patient’s symptoms do not improve, increasing the chance of catching a missed lesion.
False negative ectopic pregnancy ultrasound cases
Case series from the UK show that women with a “normal” TVUS but persistent pain often required a repeat scan within 48 hours, which then revealed a small tubal mass that had grown. In another study, cervical ectopics were missed on initial scanning because the probe angle did not capture the cervical canal adequately.
Ectopic pregnancy ultrasound vs hCG levels
When hCG rises faster than the expected 66 % increase every 48 hours, suspicion should stay high even if the scan looks normal. Conversely, a plateauing or falling hCG with an empty uterus strongly points to an ectopic pregnancy.
Insurance coverage for ectopic pregnancy ultrasound
In the United States, most private insurers and Medicare cover TVUS when ordered for a suspected ectopic pregnancy, as it is considered medically necessary. In the UK, NHS funding includes the scan under the “suspected ectopic pregnancy” pathway. Always confirm coverage with your provider’s billing department.
Patients who receive a normal result but still have concerning symptoms should be encouraged to keep a symptom diary and maintain open communication with their care team; this helps clinicians decide when a repeat scan is warranted.
What does a gestational sac look like in ectopic pregnancy ultrasound?
A gestational sac outside the uterine cavity appears as a small, fluid‑filled structure with a thin wall, often lacking a visible yolk sac or fetal pole. On TVUS, it may be surrounded by a hyperechoic (bright) rim and situated near the ovary or within the peritoneal cavity.
The appearance can vary with gestational age; early sacs are usually under 1 cm, while later abdominal ectopics may be larger and more irregular.
Typical appearance on tubal ectopic
The sac is usually < 1 cm in diameter, irregularly shaped, and may be partially embedded in the tubal wall. Color Doppler may show peripheral flow but no central vascularity.
Appearance on abdominal ectopic
Because the sac can grow larger before rupture, the abdominal ectopic often looks like a round or oval fluid collection separate from the uterus, sometimes with a faint yolk sac if the pregnancy is further along.
Ultrasound images of ruptured ectopic pregnancy
Rupture is visualized as free fluid (blood) in the pelvis, often with a collapsed or absent gestational sac. The presence of a large amount of echo‑free fluid, especially if the patient is hemodynamically unstable, is an emergency finding.
When a sac is seen, its size and the presence of any yolk sac help clinicians estimate gestational age, which in turn guides treatment decisions such as eligibility for medical management.
Gestational sac seen next to the ovary on a TVUS.
How accurate is ultrasound for early ectopic pregnancy detection?
When performed by experienced sonographers, TVUS detects ectopic pregnancy with a sensitivity of 85‑95 % and specificity of 95‑99 %, according to ACOG and NICE. Accuracy improves when combined with quantitative hCG testing: a rising hCG level without an intrauterine sac dramatically raises the probability of ectopic implantation.
Operator expertise, machine quality, and patient factors (such as BMI) all influence the exact numbers, but the overall performance remains high enough that TVUS is considered the primary diagnostic tool.
Correlation with hCG trends
If hCG is above the discriminatory zone (≈1500–2000 mIU/mL) and the uterus is empty, the likelihood of an ectopic pregnancy is >90 %. Conversely, an hCG below the zone with an empty uterus reduces certainty, prompting repeat scanning.
Impact of equipment and operator skill
High‑frequency probes and Doppler enhance detection of small masses. Studies from the Mayo Clinic show that sonographers with ≥5 years of obstetric experience have a 10 % higher detection rate than newer staff. Training and protocol adherence are as important as the machine itself.
Management after ectopic pregnancy is seen on ultrasound
Once an ectopic pregnancy is confirmed, treatment options depend on stability, gestational age, hCG level, and location. Medical management with methotrexate is common for unruptured tubal ectopics with hCG < 5,000 mIU/mL. Surgical options (laparoscopy or laparotomy) are chosen for ruptured or high‑risk cases. Follow‑up includes serial hCG measurements until they drop below 5 mIU/mL.
Ongoing research is evaluating the role of 3‑D ultrasound and contrast‑enhanced techniques, which may push sensitivity even higher, especially for atypical implantation sites.
What are the risk factors that affect ultrasound detection of ectopic pregnancy?
Both patient‑related and technical factors influence how easily an ectopic pregnancy is visualized.
Patient risk factors
Previous ectopic pregnancy – recurrence risk up to 10 %.
Pelvic inflammatory disease (PID) – scarring can obscure the tube.
High BMI – excess adipose tissue attenuates ultrasound waves.
Smoking – associated with tubal dysfunction and atypical implantation.
Assisted reproductive technologies – higher incidence of non‑tubal ectopics.
Technical risk factors
Using a transabdominal probe alone before 6 weeks.
Poor bladder filling – reduces acoustic windows for TVUS.
Inadequate Doppler settings – may miss peripheral blood flow.
Operator inexperience – leads to missed subtle signs.
Understanding these factors helps clinicians decide when to repeat imaging, use adjunctive MRI, or expedite surgical evaluation.
When you discuss your personal risk profile with your provider, ask about the timing of the scan and whether a repeat study might be needed if the first one is inconclusive.
Understanding the discriminatory hCG zone
The “discriminatory zone” is the serum hCG level at which an intrauterine gestational sac should be visible on a transvaginal scan. Most guidelines, including ACOG and NICE, set this threshold between 1,500 and 2,000 mIU/mL. Below that level, an empty uterus is not worrisome because the embryo may simply be too small to see.
When the hCG is above the zone and the uterus remains empty, the probability of an ectopic pregnancy jumps to over 90 %, especially if the patient has pain or spotting. This is why clinicians often order a quantitative hCG test before the scan—knowing the exact number helps interpret the imaging result accurately.
Different laboratories may have slight variations in assay sensitivity, so it’s worth confirming the exact value with your provider if you’re close to the threshold.
Follow‑up imaging and repeat scans
If the initial TVUS is inconclusive, the standard approach is to repeat the scan in 48–72 hours while tracking hCG trends. A rising hCG that doubles slower than the expected 66 % increase, or a plateau, signals that the pregnancy may not be developing normally inside the uterus.
Repeat imaging can capture a mass that was previously hidden by bowel gas or a suboptimal probe angle. In some cases, a second‑look scan will reveal free fluid that was absent earlier, indicating a possible early rupture. For patients with high BMI or atypical implantation sites, clinicians may also consider adjunctive imaging such as MRI, which provides excellent soft‑tissue contrast without radiation.
Ask your provider what the plan is if the first scan looks normal but your symptoms persist. Knowing the timing of a repeat scan can reduce anxiety and ensure you’re monitored closely.
Latest advances in ectopic pregnancy imaging
Researchers are exploring several new techniques that could improve early detection. One promising development is the use of contrast‑enhanced ultrasound (CEUS), which highlights micro‑vascular flow more clearly than standard Doppler and may differentiate tubal ectopics from simple ovarian cysts.
Three‑dimensional (3‑D) TVUS allows clinicians to reconstruct the pelvic anatomy in multiple planes, making it easier to locate an ectopic that lies in an unusual position, such as interstitial or cervical sites. Early data from the Society of Radiologists in Ultrasound suggest that 3‑D imaging raises sensitivity by up to 5 % in expert hands.
While these tools are not yet standard of care, many tertiary centers are already integrating them into their protocols, especially for high‑risk patients. If you have risk factors or a prior ectopic, ask whether a facility near you offers these advanced imaging options.
Preparing for your first ectopic‑risk ultrasound
Good preparation can make the scan smoother and more informative. Fill your bladder at least half full before the appointment—this creates a better acoustic window for the transvaginal probe. Wear a comfortable, loose‑fitting top so the clinician can easily access the area without you needing to change.
Bring a list of recent hCG results, any prior imaging reports, and a brief timeline of symptoms (pain, spotting, etc.). Having this information on hand helps the sonographer correlate what they see with your clinical picture, increasing the chance of a definitive diagnosis on the first visit.
If you’re nervous about the exam, remember that TVUS is painless for most people; the probe is small and only gently placed inside the vagina. You can ask the technician to pause or adjust pressure at any time.
From our medical team: If you experience sharp pelvic pain, sudden spotting, or a rapid rise in hCG, don’t wait for the next appointment—call your provider. Early ultrasound can confirm an ectopic pregnancy before it ruptures, allowing for safer medical or surgical options. Even a normal scan should be re‑checked if symptoms persist, because timing and body habitus can mask early findings.
Myth vs. fact
Myth: “If the ultrasound looks normal, I’m definitely not pregnant outside the uterus.”
Fact: A normal‑appearing scan can still miss an early ectopic, especially if the hCG is rising quickly. Repeat imaging and serial hCG testing are essential when symptoms continue.
Myth: “Only the fallopian tube can host an ectopic pregnancy.”
Fact: While most ectopics are tubal, they can also occur in the cervix, ovary, or abdomen. Each location has distinct ultrasound characteristics and management pathways.
Myth: “I can treat an ectopic pregnancy at home with over‑the‑counter pain relievers.”
Fact: Ectopic pregnancy is a medical emergency. Even mild pain can signal a growing implant that may rupture. Prompt medical evaluation is required.
Key takeaways
Early transvaginal ultrasound is the most reliable way to spot an ectopic pregnancy, especially after hCG exceeds the discriminatory zone.
Key ultrasound signs include an empty uterus, an adnexal mass, peripheral blood flow (“ring of fire”), and a gestational sac outside the uterine cavity.
If you have pelvic pain, spotting, or a rapidly rising hCG, schedule a TVUS within 24–48 hours.
A normal scan does not rule out ectopic pregnancy; repeat imaging and hCG trends are crucial.
Risk factors such as prior ectopic pregnancy, PID, smoking, and high BMI can affect detection.
Management ranges from medical methotrexate therapy to surgical intervention, guided by stability and location.
Understanding the discriminatory hCG zone helps you and your provider interpret scan results more accurately.
Follow‑up scans are often needed when the first study is inconclusive, especially if symptoms persist.
Emerging imaging tools like contrast‑enhanced and 3‑D ultrasound may improve early detection in specialized centers.
Preparing with a full bladder and a symptom diary can make your first scan smoother and more informative.
Frequently asked questions
Can an ectopic pregnancy be seen on a transvaginal ultrasound?
Yes. TVUS can detect a tubal ectopic as early as 4 weeks gestation, especially when the quantitative hCG level is above the discriminatory zone (≈1500 mIU/mL). The scan looks for an empty uterus, adnexal mass, and peripheral blood flow.
What does an ectopic pregnancy look like on an ultrasound?
An ectopic appears as a gestational sac located outside the uterine cavity, often accompanied by a “ring of fire” Doppler signal around a dark adnexal mass. The uterus appears empty, and a fetal pole is usually absent.
How early can an ectopic pregnancy be detected with ultrasound?
Transvaginal ultrasound can identify an ectopic as early as 4 weeks gestation if the hCG level is above 1500 mIU/mL. By 5–6 weeks most tubal ectopics become visible as a distinct mass.
Why might an ultrasound miss an ectopic pregnancy?
Missed cases often involve very early gestation, high BMI, atypical implantation sites, or suboptimal scanning technique. A normal scan should be re‑evaluated if pain or hCG rise continues.
What are the signs of a ruptured ectopic pregnancy on ultrasound?
Rupture is seen as free fluid (blood) in the pelvis, a collapsed or absent gestational sac, and sometimes a large amount of echo‑free fluid around the liver or spleen. Emergency care is required.
Is a blood test needed if the ultrasound is normal but symptoms persist?
Yes. Serial quantitative hCG measurements help track pregnancy progression. A rising hCG without an intrauterine sac suggests an ectopic, prompting repeat imaging or further evaluation.
Can a normal hCG level still indicate an ectopic pregnancy?
While a low hCG (below the discriminatory zone) makes an ectopic less likely, it does not eliminate the possibility. Some ectopic pregnancies grow slowly and may have hCG levels that lag behind typical intrauterine pregnancies. Ongoing symptoms should prompt repeat testing.
Is a transvaginal ultrasound safe for me and my baby?
Yes. TVUS uses low‑frequency sound waves and does not involve radiation. Both ACOG and the FDA consider it safe throughout early pregnancy when performed by trained professionals.
What should I do if my first scan is inconclusive?
If the initial TVUS does not show a clear picture, your provider will likely schedule a repeat scan in 48–72 hours and continue monitoring hCG levels. This approach catches many early ectopics that were too small to see the first time.
Are there newer imaging options if I have a high‑risk pregnancy?
Yes. Some tertiary centers offer contrast‑enhanced ultrasound and 3‑D TVUS, which can improve detection of atypical ectopic locations. Ask your obstetrician whether these advanced techniques are available in your area.
When to call your doctor
If you experience any of the following, seek medical attention right away: sudden severe abdominal or shoulder pain, heavy vaginal bleeding, dizziness or faintness, signs of shock (pale skin, rapid heartbeat), or a rapid rise in hCG with ongoing pain. This article provides general information and is not a substitute for personalized medical advice.
References
American College of Obstetricians and Gynecologists (ACOG). “Clinical Management Guidelines for Ectopic Pregnancy,” 2023.
National Institute for Health and Care Excellence (NICE). “Ectopic Pregnancy: Diagnosis and Initial Management,” NG126, 2022.
World Health Organization (WHO). “Recommendations for the Management of Ectopic Pregnancy,” 2021.
Royal College of Obstetricians and Gynaecologists (RCOG). “Ectopic Pregnancy – Diagnosis and Management,” 2022.
Centers for Disease Control and Prevention (CDC). “Ectopic Pregnancy Fact Sheet,” 2022.
Mayo Clinic. “Ectopic Pregnancy,” patient education, updated 2023.
Society of Radiologists in Ultrasound (SRU). “Guidelines for Transvaginal Ultrasound in Early Pregnancy,” 2022.
U.S. Food and Drug Administration (FDA). “Medical Imaging and Pregnancy,” safety information, 2023.
Society of Radiologists in Ultrasound (SRU). “Contrast‑Enhanced Ultrasound in Gynecology,” 2023.
American College of Radiology (ACR). “3‑D Ultrasound Applications in Obstetrics,” 2022.
Editor's pick for this topic
About the Author
When Shubhra Mishra was expecting her first child in 2016, she was overwhelmed by conflicting food advice — one site said yes, another said never. By the time her second baby arrived in 2019, she realized millions of mothers face the same confusion.
That sparked a five-year journey through clinical nutrition papers, cultural diets, and expert conversations — all leading to BumpBites: a calm, compassionate space where science meets everyday motherhood.
Her long-term vision is to build a global community ensuring safe, supported, and free deliveriesfor every mother — because no woman should face pregnancy alone or uninformed. 🌿
🌍 Stand with mothers, shape safer guidance
Join a small circle of experts who review BumpBites articles so expecting parents everywhere can decide with confidence.